Cubital tunnel syndrome
The body contains many nerves that provide essential signals from the brain and central nervous system, instructing other bodily parts to perform various tasks. One specific nerve is the ulnar nerve.
When the ulnar nerve is subjected to illness or injury, people can develop a medical condition known as ulnar neuropathy.
Cubital tunnel syndrome generally occurs from prolonged pressure on the nerve, usually caused by keeping the elbow bent for too long or from moving it too much and too vigorously for long periods. Both nonsurgical and surgical options are available to help get you back to your day-to-day activities. Surgical procedures are only recommended when nonsurgical treatments are ineffective. It is important to see a Florida Orthopaedic Institute physician as quickly as possible to prevent the condition from worsening to the point when the hand muscles begin to die and cannot be regained (muscle wasting).
Anatomy
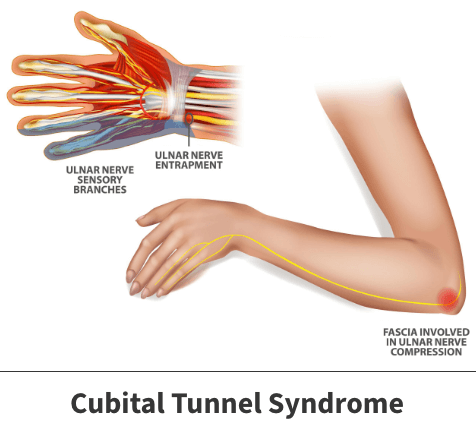
The ulnar nerve is one of the arm’s primary nerves. It begins in your neck, travels through the arm, and ends in the hand. The ulnar nerve plays a significant part in your ability to move your wrist, hand, and fingers. It also gives feeling to the little finger and half of the ring finger while also controlling most of the small hand muscles, as well as some bigger muscles in the forearm. It travels through a tunnel of tissue called the cubital tunnel, which runs under a bump of bone at the inside of the elbow, known as the medial epicondyle. This area of the elbow is commonly known as the funny bone, which causes a shock-like feeling when bumped because the nerve is so close to the skin.
About
Cubital tunnel syndrome, sometimes called ulnar nerve entrapment, happens when the nerve has pressure against it. This pressure, known medically as a constriction, can irritate or inflame the nerve. Such events can occur at any point along the nerve. The most common problematic site is the inside of the elbow.
Causes
Several locations throughout the arm can compress the ulnar nerve, such as the collarbone or wrist. But the most common place for the ulnar nerve to be compressed is behind the inside part of the elbow. When this occurs, it results in a condition known as cubital tunnel syndrome. Several factors that can cause pressure on the nerve at the elbow have the potential to lead to cubital tunnel syndrome:
- Repetitive movements – Over time, the repeated bending and twisting of the arm, wrist, and elbow may weaken the nerve and lead to irritation.
- Nerve misalignment – Occasionally, the ulnar nerve may shift out of position. This continual back-and-forth movement may result in irritation.
- Acute trauma – Sudden events in which the arm experiences forceful contact could result in ulnar nerve irritation or damage. Specific incidents include falls, automobile accidents, and sports involving strong and consistent physical interaction.
- Fluid buildup – Certain occurrences might cause tissues surrounding the nerve to collect with fluid. When this problem grows large enough, the pressure produced can press against the nerve.
- Extended idle time – Leaving the arm or elbow in the same position for long times can place unnecessary strain on the ulnar nerve.
- Illness – Any type of illness capable of damaging or weakening nerves or surrounding tissues can eventually result in cubital tunnel syndrome.
Risk factors
An individual’s risk of developing the issue increases when one has experienced previous injury or illness within their arm, competes in contact sports, or works a job requiring repetitive or unusual arm motions. Sometimes an accessory muscle or increased laxity to connective tissue may cause ulnar neuropathy at the elbow.

Symptoms
Symptoms may vary depending on how severe the nerve compression is and where along the nerve the problem exists. Those with cubital tunnel syndrome often deal with occurrences like:
- Difficulty moving their hands or fingers
- Elbow pain
- Numbness and tingling in the ring and little fingers
- The feeling of falling asleep in the ring and little finger, mostly when the elbow is bent.
- A weakening of the grip
- A decrease in finger coordination
- If the nerve has been compressed for an extended period, muscle wasting in the hand can occur. Muscle wasting is when the muscle starts to die and cannot come back.
In many instances, these symptoms start and stop. In severe cases, such occurrences might limit the person’s mobility and interfere with their ability to perform routine tasks.
Complications
If the issue is not identified and treated as early as possible, one might experience irreversible damage in the neighboring arm and hand components like muscles.
Treatment
Both nonsurgical and surgical treatments exist. Typically, your doctor will prescribe nonsurgical methods and only recommend surgery in the most severe cases or those not responding favorably to less aggressive measures.
Nonsurgical treatment options
There are several nonsurgical treatment options available for cubital tunnel syndrome. Your physician may recommend some or all of the following:
- Non-steroidal anti-inflammatory medicines – Medications like Advil & Motrin (ibuprofen) and Aleve (naproxen) may be recommended, which can help reduce swelling around the nerve. They should only be used as directed and not for extended periods unless directed by your healthcare provider.
- Nerve gliding exercises – Exercises to help the ulnar nerve slide through the cubital tunnel at the elbow can improve symptoms. These exercises can also help prevent stiffness in the arm and wrist.
- Bracing or splinting – Your physician may prescribe a padded brace or splint to wear at night to keep your elbow straight, decreasing pressure. This often proves especially effective in preventing movement during sleep.
- Occupational therapy. Occupational therapists can teach you proper hand motion techniques to limit incidents of ulnar nerve concerns.
Surgical Procedures
Your Florida Orthopaedic Institute physician may recommend a surgical treatment to take the pressure off the nerve if nonsurgical methods have not improved your condition, the ulnar nerve is very compressed, or if nerve compression has caused muscle weakness or damage. The surgical treatments currently available include:
- Cubital tunnel release – During this procedure, the ligament “roof” of the cubital tunnel is cut and divided, increasing the tunnel’s size while decreasing pressure on the nerve. As the ligament heals, new tissue grows across the division, expanding the tunnel. This procedure works best when the nerve does not slide out from behind the bony ridge of the medial epicondyle when the elbow is bent.
- Ulnar nerve anterior transportation – Unlike cubital tunnel release, this procedure corrects the nerve’s location if it has slid out from behind the bony ridge of the medial epicondyle. During this procedure, the nerve is moved to lie either under the skin but on top of the muscle (subcutaneous transposition), under the muscle (sub-muscular transportation), or within the muscle (intermuscular transportation).
- Medial epicondylectomy – This procedure removes part of the medial epicondyle, releasing the nerve. This technique will prevent the nerve from getting caught on the boney ridge of the medial epicondyle and stretching when your elbow is bent.
Recovery
It is difficult to list exact time frames for recovery. Everyone progresses at their own rate. An individual’s recovery period will be influenced by other factors such as their age, overall health, physical activity level, the specific problem causing the ulnar nerve compression, that issue’s severity, and the method used to treat it.
It is important to remember that nerves usually improve at a slower pace than other physical features. It might take several months before recovery occurs.
Prevention
One may avoid cases of cubital tunnel syndrome or reduce their risk by not leaning on their elbows for long periods, limiting the amount of pressure placed on their arms, not sleeping on their elbows, and attempting not to bend their arms for extended intervals or at strange positions.
Videos
Related specialties
- Arthroscopic Debridement of the Elbow
- Aspiration of the Olecranon Bursa
- Elbow Bursitis
- Elbow Injuries & Inner Elbow Pain in Throwing Athletes
- Golfer's Elbow
- Growth Plate Injuries of the Elbow
- Hyperextension Injury of the Elbow
- Little Leaguer's Elbow (Medial Apophysitis)
- Olecranon Stress Fractures
- Radial Tunnel Syndrome
- Tennis Elbow Treatment
- Tricep Pain & Tendonitis
- UCL (Ulnar Collateral Ligament) Injuries
- Valgus Extension Overload