Valgus extension overload
Valgus Extension Overload (VEO), also known as throwers arm, happens when the elbow is overused, resulting in deterioration and the development of bone spurs. VEO also causes pain, swelling, and possible numbness. While it is possible for anyone to get VEO, throwing athletes are most vulnerable. Both surgical and nonsurgical treatment options are available and able to eliminate symptoms while allowing athletes to return to their sport as quickly as possible.
Anatomy
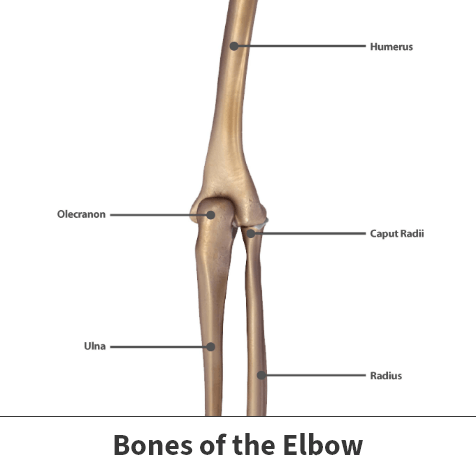
The elbow joint is where the upper arm bone (humerus) meets the two forearm bones (radius and ulna). The bony point of the elbow (olecranon) is at the upper end of the ulna.
The joint consists of several muscles, ligaments, nerves, and tendons, and is both a pivot and hinge joint, meaning it allows you to bend and straighten, as well as twist and rotate your arm. Thick ligaments (collateral ligaments) are located on the inner and outer sides of the elbow and hold the joint together while preventing dislocation. The ulnar collateral ligament (UCL) is found on the inside of the elbow and runs from the inner side of the humerus to the inner side of the ulna. The ulnar nerve crosses behind the elbow and controls the muscles of the hand and provides sensation to the small and ring fingers.
About
During a throwing motion, the elbow undergoes extreme stress; the humerus and olecranon get pushed and twisted against each other while the UCL works to stabilize the whole joint. This repetition of movement and extreme stress on the elbow can lead to the deterioration of the protective cartilage on the olecranon, resulting in the development of abnormal overgrowth of bone (bone spurs/osteophytes). This condition is known as Valgus Extension Overload (VEO).
VEO is not an acute injury (one that happens instantaneously) – it occurs gradually over time from overusing the elbow. Since VEO is the result of overuse and the repetitive high stress of throwing, it is very uncommon for non-throwers to get this injury.
Symptoms
VEO is most common in athletes, specifically throwing athletes.
Symptoms include:
- Pain during or after throwing
- Limited throwing ability
- A decrease in throwing speed
- Frequent numbness and tingling of the elbow, forearm, or hand

Diagnosis
Your Florida Orthopaedic Institute physician will examine your range of motion, strength, stability of the elbow, sensation, muscle bulk, appearance, and possibly even your shoulder. They will use all this information to pinpoint the exact location of pain. A valgus stress test will be performed, which recreates the stresses placed on the elbow while throwing. During the test, your physician will hold your arm while applying pressure against the side of the elbow. More testing may also be needed to make sure that you have VEO and not a different injury:
- X-rays – X-rays will often show stress fractures, bone spurs, and other abnormalities.
- Computed tomography (CT) scans – CT scans provide three-dimensional images of the bone and can be very helpful in defining bone spurs or other bony disorders that are found in VEO.
- Magnetic resonance imaging (MRI) scans – MRI scans provide a view of the soft tissues of the elbow, which can assist in distinguishing between ligament and tendon disorders that often have the same symptoms as
VEO testing can also help determine the severity of an injury, such as whether a ligament is mildly damaged or completely torn, and can identify a stress fracture that is not visible in an X-ray image.
Treatment
In most cases, VEO can be eliminated with rest and physical therapy. If physical therapy does not improve pain, there are several surgical procedures that can be performed to eliminate pain.
Nonsurgical treatments
In most cases, the initial step to VEO recovery is a short period of rest. If there is little to no pain relief, then more treatment options will be required. These treatments include:
- Physical therapy – Strength and flexibility can be restored with specific exercises. Your Florida Orthopaedic Institute physician will design a rehabilitation program that will allow for a gradual return to throwing.
- Medications – Ibuprofen (Motrin) and naproxen (Aleve) reduce swelling and pain and can be provided in prescription-strength form.
- Change of position – Your throwing form can be evaluated and corrected to lessen the excessive stress on the elbow.
Although a change of position or even a change of sport can reduce if not completely eliminate the repetitive stress and pain caused by throwing, it is often an unwelcome option, especially in high-level athletes. Athletes would rather not change how they play or quit their sport.
Surgical procedures and treatments
There are several surgical procedures that can eliminate VEO without forcing an athlete to alter their playing ability, including:
- Bone spurs on the olecranon, as well as any loose fragments of bone or cartilage within the elbow joint, can be removed arthroscopically. During this procedure, the surgeon inserts a small camera (arthroscope) into the elbow joint, allowing the inside of the elbow to be projected on a screen. The surgeon uses this projection to guide miniature surgical instruments. The arthroscope allows for a small cut rather than the larger ones needed for standard open surgery.
Recovery
If nonsurgical treatment is successful, the athlete can often return to throwing in approximately 6 to 9 weeks. If surgery is required, the recovery time is dependent on the procedure performed and the severity of the injury.
Recent research focusing on VEO prevention has determined that proper conditioning, technique, and recovery time can help to prevent throwing injuries in the elbow. As for younger athletes, pitching guidelines such as the number of pitches per game and week, as well as the type of pitches thrown can protect children from VEO as well as other injuries in the future.
Related specialties
- Arthroscopic Debridement of the Elbow
- Aspiration of the Olecranon Bursa
- Cubital Tunnel Syndrome
- Elbow Bursitis
- Elbow Injuries & Inner Elbow Pain in Throwing Athletes
- Golfer's Elbow
- Growth Plate Injuries of the Elbow
- Hyperextension Injury of the Elbow
- Little Leaguer's Elbow (Medial Apophysitis)
- Olecranon Stress Fractures
- Radial Tunnel Syndrome
- Tennis Elbow Treatment
- Tricep Pain & Tendonitis
- UCL (Ulnar Collateral Ligament) Injuries